
 Farsi (فارسی)
Farsi (فارسی) Kurdish (کوردی)
Kurdish (کوردی)
In the Name of Traditions: A Comprehensive Study on the Impact of Female Genital Mutilation (FGM) on Women and Girls
An Overview of Female Genital Mutilation (FGM) in Iran
Abstract
A comprehensive study was undertaken to investigate, explore and analyse the existence of female genital mutilation/cutting (FGM or FGM/C) in Iran. The timespan of this study began in 2005 and ended in 2014. The aim of this study was to provide in-depth data on FGM in Iran and, at the same time, provide the building blocks for a comprehensive programme to combat FGM in Iran and bring this issue onto the world’s agenda. The methodological approach adopted by this study was primarily participatory, due to the sensitivity of the subject matter. Most parts of this research were completed by the end of 2014, and much has been achieved over a decade of studying the subject of FGM in Iran.
The study included travelling thousands of kilometers and interviewing over 3,000 women and 1,000 men from various areas and social classes, including key role players, community leaders, clerics and religious leaders in order to compile comprehensive data about the practice of FGM in Iran. The findings demonstrate that FGM in some locations is widespread among women and girls (around 60% in some villages of Qeshm Island in the southern province of Hurmozgan, especially in the villages of the four provinces in the north-west, west and south of Iran). FGM was not, however, practised in the northern parts of West Azerbaijan, where people are Turkish Azeri and Kurmanji Kurdish speakers, nor in the southern parts of Kermanshah and northern parts of Hormozgan.
This research study, along with a short documentary film, has gained global recognition and was launched by The Guardian and the BBC on 4 June 2015 through their websites. Shortly thereafter it was discussed at a United Nations meeting of the Human Rights Council in Geneva, on 19 June 2015 at a session on eliminating FGM. Reuters also published an analysis of the research and considered it one of the rare contributions in the history of Iran.
Introduction
Combating female genital mutilation (also known as female genital cutting – FGM or FGC) is a controversial subject globally, and its elimination is considered imperative by feminists, human-rights campaigners and social activists as well as international organisations such as UNICEF and responsible governments. The practice generally involves the partial or, in some extreme cases, the total removal of the external parts of female genitalia. In English, the term ‘female circumcision’ has been used for this practice, to compare it with male circumcision. Nowadays, however, as a result of the work of feminist activists against this practice, ‘female genital mutilation’ (FGM) is the preferred expression. An extreme form of FGM can have serious health consequences for a girl, including traumatisation and even, in some cases, death due to severe bleeding and infections. In the long term, women who have been subjected to FGM suffer undesirable health effects in their lives, especially in marriage.
Recent data from the United Nations Children’s Fund (UNICEF) indicates that roughly 130 million girls and women alive today, worldwide, have undergone some form of FGM (UNICEF 2014). Further research shows that 92 million of them are over the age of ten and most live in Africa. According to official UN data, FGM is practised in 29 countries in western, eastern, and north-eastern Africa, in parts of the Middle East and Asia, and within some immigrant communities in Europe, North America and Australia (EndFGM 2012, UNICEF 2013). Its prevalence in several countries exceeds 80% (UNICEF 2014). The age of girls undergoing FGM varies from one culture to another. In general, it is performed on a girl between the ages of 4 and 12; however, in some cultures it is practised on new-borns or just prior to marriage.
FGM is a longstanding ritual that continues to violate aspects of women’s sexual rights. It prevails in societies because of certain beliefs, norms, attitudes, and political and economic systems. While there is some data available on FGM in Iran, it is limited in scope. This research has, for the first time, given a complete overview of the prevalence of FGM in the whole of Iran, with a focus on the most FGM-affected areas in the western provinces West Azerbaijan, Kurdistan and Kermanshah, and in some areas of southern Hormozgan province and its islands.
Objectives of the Research Study
The central objective of the current research study was to benefit communities with its findings and recommendations and to give the Government, individuals and NGOs large, updated, authentic datasets about the existence of FGM in Iran.
The findings of the study contribute to two larger perspectives. Firstly, it works as a baseline for future studies and research in Iran, which is required; secondly, it will help create and increase awareness about the presence of FGM, to focus the attention of the Iranian Government on its international liabilities and responsibilities.
More broadly, the research also refutes the longstanding belief that Africa is the only continent where FGM takes place, and at the same time provides enough evidence to ensure that FGM is never again denied in Iran. Exposing this data will assist Iranian society, children’s-rights lobbies and international organisations in starting dialogues with the relevant stakeholders to help address and combat FGM in Iran.
The study introduces FGM along with the well-known justifications given by communities that practise it. Besides revealing the truth about the practice of FGM in Iran, this study discusses historical perspectives on the ritual, the prevalence of the practice across the region and the globe, the emerging reduction in the occurrence of FGM, and the range of beliefs and reasons underlying it. It also highlights the number of practices/programmes adopted so far to tackle the issue in the specified areas of Iran. The report also considers the historical fight against FGM; some legislative measures against it; the role of clerics, the community and governments; and, most importantly, men’s perceptions in this regard.
Historical Perspective and Global Prevalence
In most cultures, talking about women’s sexuality is a taboo, and for that reason it is difficult to get precise information on the historical roots of the ritual of FGM. The origins of FGM are not precisely known, although historians and anthropologists have done much research on the topic. Several sources have traced it back more than 2,000 years and generally point to ancient Egypt, specifically areas around the Nile, as its geographical heartland, from where it spread (Slack 1988). Some historians claim that it is a pharaonic practice and that its roots lie in 5th century BC Egypt.
Anthropologists mention it as an African Stone Age way of ‘protecting’ a young female person from rape (Lightfoot-Klein 1983). Some research has linked it with early 17th century Somalia, where it was carried out to get a better price for female slaves, and with an Egyptian practice to prevent pregnancies in women and slaves (Lightfoot-Klein 1983). The early Roman and Arabic civilisations linked FGM with virginity and chastity; in ancient Rome female slaves were made to undergo it to oppress sexual activity and to raise their values (Tankwala 2014).
It is well known that FGM was traditionally practised in many parts of the world and is not limited to Africa and the Middle East. It was practised by Australian Aboriginal communities (Harris-Short 2013), the Phoenicians, the Hittites, the Ethiopians (Rahman and Toubia 2000), and ethnic groups in Amazonia, some parts of India, Pakistan, Malaysia, Indonesia, and the Philippines (Guiora 2013). In the 19th century, FGM was practised in Europe and the US, where some physicians embarked on clitoridectomy to prevent masturbation or counteract female homosexuality and some mental disorders such as ‘hysteria’ (Brown 1866). In fact, FGM sporadically continued in the USA until the 1970s in one form or another.
FGM predates Islam and Christianity; however, most communities that perform FGM are Muslim, and so religion is frequently cited as a reason for its continuation (Bob 2011). Nonetheless, Islamic scholars do not all agree with this notion and some condemn the attachment of the practice to Islam. FGM also occurs among small groups of Christians, animists, and Jews and members of other indigenous religions (Bob 2011, Nyangweso 2014); for example, in Eritrea and Ethiopia, Coptic and Catholic Christian communities practise FGM. In the Jewish groups Beta Israel and Falasha, FGM is widespread (Favali and Pateman 2003).
According to UNICEF data, FGM is most common in 29 countries in Africa, as well as in some countries in Asia and the Middle East and among certain migrant communities in North America, Australasia, the Middle East and Europe (UNICEF 2013). There is no evidence for it in southern Africa or in the Arabic-speaking nations of North Africa, except Egypt (Toubia 1995). Increased migration of people from practising countries has resulted in the spread of FGM to other parts of the world, including Australia, Canada, New Zealand, the US and European nations (Boyle 2005). The practice can also be found to a lesser extent in Indonesia, Malaysia, Pakistan and India (Isiaka and Yusuff 2013). In Iraq, FGM is practised among Sunni Kurds, some Arabs, and Turkmens. A survey done by a number of NGOs in 2005 suggests 60% prevalence among Kurds in Iraq (Ghareeb and Dougherty 2004, 226). Later studies from the same area, following the launch of a number of local and regional campaigns to combat FGM, suggested a lower rate. According to the Kurdish Regional Government, UNICEF and local NGOs, FGM rates have been dropping rapidly.
Reliable figures on the prevalence of FGM are increasingly available. A statistical review by UNICEF mentions that national data have now been collected in the Demographic and Health Survey Program (DHS) for six countries: the Central African Republic, Côte d’Ivoire, Egypt, Eritrea, Mali and Sudan. In these countries, the rate among reproductive-age women varies from 43% to 97%. Data for these countries also subdivide the rates among different ethnic groups. However, the statistics have, until recently, been silent about FGM’s presence in the US and a few other Western countries (UNICEF 2013). Iran is now also on the list of practising countries.
Background of the Research Study
This paper is based on a study that attempted to identify the prevalence of FGM in Iran and investigated the role of diverse contributing factors. In 2005, a field study in a number of neighbouring regions began, and, at the same time as the data was collected, a documentary was made from the interviews and related footage.
The first and only (publicly available) documentary about FGM in Iran, In the Name of Tradition was filmed in the Kurdish villages and neighbourhoods of Mahabad, in some villages of the nearby Kurdistan province, in regions of Hawraman in Kermanshah province, and in Hurmozgan province in the south of Iran (Ahmady 2006). This anthropological documentary contains recorded footage and interviews from the regions and villages of Kermanshah and Hormozgan province and from its islands (e.g. Qesham, Hormozgan, and Kish). As well as interviewing local women and female cutters (bibis; i.e. professional cutters), the documentary records the opinions of local men, medical staff, doctors and clerics.
Based on the findings of the film, it was clear that there was a need for further research to examine FGM systematically in Iran, especially in the geographical pockets where there is a high prevalence. A scientific, country-wide research project was therefore started. Local resources were required to carry out such a comprehensive study; training was provided for a number of young, enthusiastic male and female students and individuals who were willing to participate and conduct most of the face-to-face field interviews. UNICEF-style standardised questionnaires were used to collect data.
Evidence from the preliminary research and documentary indicated that FGM is less likely to occur in towns; the focus of the research was therefore rural areas. Initially, villages were picked randomly from predefined geographical positions in the north, west, east and south. However, as the research progressed, more comprehensive, village-by-village training and pilot projects were implemented. As the fact-finding mission progressed and more areas from each province were visited and samples taken, the research teams were led to neighbouring villages and regions and, finally, to the south of Iran and the province of Hormozgan, where the rate of FGM is highest.
Maps, local guides, clerics and personal connections were utilised throughout the study. The research was conducted over the span of ten years by a small, but very enthusiastic group. Since the study was not a full-time project and was conducted during different seasons, the initial fact-finding mission, field work and training took place between 2005 and 2015. The study employed multiple approaches such as different phases, strategies, methods, and tailor-made training manuals to fit the various tastes and languages of each region. A number of pilot programmes were run in different regions to the east and west, where face-to-face visits with community stakeholders took place.
Awareness-raising sessions, using different approaches, mainly with young women, were arranged to highlight the dangers of FGM on female bodies and human lives. The sensitisation of men was also part of the approach. The team engaged with groups of men in mosques, houses, and many public places to measure levels of success. Different sessions of lobbying were held with community leaders and, most importantly, with clerics and local women as well as local and regional Sheiks to gain their support for banning FGM and issuing local fatwas. After each piece of fieldwork and face-to-face training/lobbying, follow-up visits to the same villages were carried out twice and one year later to assess the success and impact of the pilot programmes.
Research Methodology
International data on FGM have been collected through a separate module of the Demographic and Health Surveys Program (DHS) since the beginning of 1990. The module has yielded a rich dataset comparable over many countries, mainly in Africa. Since the prevalence of FGM in Iran has not been addressed by UN/UNICEF or any other international organisation, a module similar to that of the DHS’s was used to conduct the first ever country-wide data-collection project.
The methodological approach adopted by this study was primarily participatory, due to the subject matter. This methodological framework took into account the views of women and girls, in particular those of actual victims, so that the findings would reflect their true views. The language of the interviews was simple and user-friendly to avoid any ambiguity or misunderstandings between participants. Since the research stretched over a period of ten years, the methodology was adjusted along the way as we came up with new strategies.
UNICEF-style standardised questionnaires were used to collect data in the style of the DHS and UNICEF’s Multiple Indicator Cluster Surveys (MICS). Importantly, good communication and networking allowed the researchers to win support from the local population, some community and religious leaders, and a number of academics. Local individuals were chosen for the work, the aim being to ensure they adhered to ethical standards and maintained confidentiality. As May puts it, ethical standards in research ‘are binding, hence need to be adhered to irrespective of the circumstances surrounding the research; they remind us of our responsibilities to the people being researched’ (May 2011). She adds that it is easier for participants, also, if they can take part with peace of mind, having all the relevant information about the research (May 2011).
For this research, participants were asked for their consent and were informed prior to the commencement of the research how the data would be utilised and what we aimed to achieve with the findings. In some cases, interviews were conducted over the phone rather than in person, applying the same standards. A total of 4,000 interviews were carried out in the provinces of Hormozgan, West Azerbaijan, Kermanshah, and Kurdistan. In each province, 1,000 interviews were conducted, involving 750 women and 250 men. For the first time in Iran, there was a focus on the male perspective to examine their role in the perpetuation of FGM. However, getting female opinions was a bit tricky due to the conservative nature of the area and the sensitivity of the research topic.
FGM in Iran: A Detailed Display of Findings
Chart 1 below gives an overview of the number of women who have undergone FGM, broken down by age, in our chosen four provinces. For uniformity in result, a number of villages per province were selected for the research.
The results clearly show the regional differences in FGM prevalence. Chart 1 shows that the percentage of women who have been cut is high in Hormozgan province, where it can reach 60% in some of the villages of Qeshm, Hormuz, and Larak islands. It is at its lowest in villages of Parsian, at 31%; northern parts of the province were FGM free. Kermanshah province had the second-highest prevalence, of 41% in villages of Paveh. However, in Kurdistan and West Azerbaijan, the numbers are comparatively low.
Analysis shows that the proportion of women in the 30–49 age bracket who have been cut is higher than that of women and girls aged 15–29. In Hormozgan and Qeshm Island, the prevalence of FGM among women aged 29–49 reaches 61%; on the other hand, it appears to have been eliminated in Sahneh/Lakastan in Kermanshah, where we found no evidence of it among women and girls aged 15–29.
These findings demonstrate an encouraging trend of FGM decreasing in all four provinces. For instance, in Piranshahr, West Azerbaijan, the rate is less than 10% among the younger generation. Similarly, in Javanrood in the same province, there is a sharp decline from 41% in older women to 9% in younger women and girls. In some of the villages of Ravansar, it again drastically decreased to 17% from 43%.


Generational Trends
The inverse relationship between age and FGM prevalence reveals that women who have undergone FGM know the suffering this practice brings. Our feedback indicated that the new generation are aware and have their own thinking about how to lead their lives. Therefore, when a couple gets married, they prefer their daughters not to suffer the way women of previous generations did.
Data were gathered through separate analytical questions to analyse the attitudinal change of mothers towards FGM over time. The findings of the survey revealed a big change in favour of ending FGM. Chart 3 shows the ratio of women who have undergone FGM aged 15–49 who have at least one daughter who has been cut. The difference between the 15–29 and 30–49 age brackets is very prominent in Kermanshah, where we see a decline of almost 90% in Javanrood and Ravansar; and around 50% in Paveh. As mentioned earlier, we found no evidence of FGM in the 15–29 age bracket in Sahneh/Lakastan, and the same applies in Sarpol e Zaheb. In Hormozgan province, the data show about a 50% decrease; in West Azerbaijan, roughly a 90% decrease between the generations was noted. Kurdistan also mirrored Hormozgan, showing a decrease in excess of 90% in some areas.
It is pertinent to mention that the following data reflects those mothers who had the opportunity to cut their daughters and refused. There were also a large number of women who mentioned that their other daughters were still too young, but that, once they reached an ‘appropriate’ age, they would undergo FGM.


Per the guidelines of the DHS and MICS, data were collected to examine the relationship between the educational attainment of mothers and FGM prevalence in their daughters. Chart 5 shows the significant impact of having an educated mother on whether a girl is subjected to FGM or not.
It can be seen through the available findings that a woman’s educational attainment is one important factor in whether or not her daughter will undergo FGM. The research and conversations with women revealed that momre highly educated women prefer not to victimise their daughters in this way; the lower a woman’s educational attainment, the more likely she is to follow tradition blindly, considering it a social norm or religious duty. Some highly educated mothers have had one of their daughters cut, although the rate is vanishingly small (or nonexistent) in four of the provinces. The data collected from the Kurdish region suggests that the practice is in decline due to a higher level of education among women.
The findings also show that highly educated women are less likely to support FGM generally, with fewer than 20% of those surveyed doing so. However, for such attitudes to make a practical difference, empowerment of women is also required.


Impact of Religion
Previous studies and the underlying research found that FGM as a ritual performed by a majority of Sunni minorities in Iran. Though it is a myth, most of the world considers FGM to be an Islamic practice; however, even within Islam there is division in opinions on its practice. For Shias, who are the majority in Iran (the official religion of Iran is also based on Shia faith), this is a practice related to the Sunni sect. They refused to consider this a part of their religious obligations.
Therefore, the prevalence of FGM is very low in the Shia population. The findings of the study into the prevalence of FGM in different sects clearly indicate that Shias in Kurdistan do not practise FGM; in West Azerbaijan, only 2% of Shias do, in Shahindej villages. In Sahneh and Sarpol e Zahab villages, the rates are 4% and 5%, respectively, among Shia. In Hormozgan province, minimal traces of FGM were recorded in Shia communities in selected villages, which shows that, though minimal, FGM is a part of Shia people’s culture in Hormozgan.

Impact of Household Wealth
Poverty is closely linked with the practice of FGM in Iran. In order to measure the impact of financial status, DHS and MICS questionnaires were used to gather information on household assets and household ownership, along with characteristics of dwellings, such as sanitation facilities used and access to safe drinking water. Each asset was assigned a weight, and individuals were ranked according to the total score of the household in which they reside.
FGM prevalence appears to fall among women from families with wealthy backgrounds, but the relationship between household wealth and FGM is not always consistent. Overall, as Chart 8 shows, FGM prevalence appears to be lower among women from families with wealthy financial backgrounds. In all four provinces, the prevalence of FGM among richer women was less than 15%.
The findings revealed that, in the selected four provinces, there is homogeneity in terms of prevalence of FGM among wealthy households. Only in Mariwan villages in Kurdistan and Paveh villages in Kermanshah were the rates higher, at 23% and 19%, respectively, among wealthy households, while in the rest there was less than a 15% occurrence among richer women. An improved financial status makes it easier for families to access better lives, education, exposure to messaging, and knowledge; therefore, their perceptions about life and practices are different. However, some among the wealthy still adhere to FGM.


Roles of Men’s and Women’s Perceptions in FGM
It is important to discover how the men’s and women’s perceptions of FGM influence its survival and who plays a prominent role in making decisions to go ahead with FGM. The research used gender-focused questionnaires to try to get at the facts. The data show that the most prominent figure in determining whether a girl is subjected to FGM is female, mostly the mother or grandmother, but sometimes another female relative; men have some say in this, but not a dominant one.
As for general support for FGM, the figures show that, in Hormozgan, support is felt by up to 44% of women in Qeshm, Hormoz, and Larak islands, while the corresponding level among men is 33%. In Paveh and Javanrood in Kermanshah, support is lower at 21% of women and less than 10% of men.
The results show that, despite the patriarchal nature of society, men appear less concerned about FGM than women. However, many women feel a silent pressure from the patriarchy and so are compelled to continue the ritual.


Influence of the Type of FGM Practitioner
Another contributing factor to the perpetuation of FGM is the vested interest of the cutters who are available within each community and the financial rewards they receive. FGM in Iran is performed by three types of people: Roma groups, bibis (midwives) and family members (in practice, older women).
The scenario in every province is distinctive. In Hormozgan, FGM is mostly performed by traditional practitioners, including bibis; however, in some areas or situations, family members may get involved. In West Azerbaijan, FGM is mainly performed by Roma groups who illegally cross from Iraqi Kurdistan into Iranian Kurdistan and West Azerbaijan province. They stay in the area for most of spring and summer, but fear arrest from the Iranian border police and keep away from towns and large cities (due to not having passports/visas). These groups are making good money by carrying out FGM in the area. Mostly, they do not use safe methods, which causes multiple types of disease. Besides Roma groups, a mix of cutters have been found among family members and traditional practitioners. In Kermanshah and Kurdistan villages, FGM is carried out by traditional practitioners, although, in some villages, Roma groups and bibis are active. They perform FGM with a razor or knife, without anaesthesia; there is no concept of medicalised and hygienic cutting.


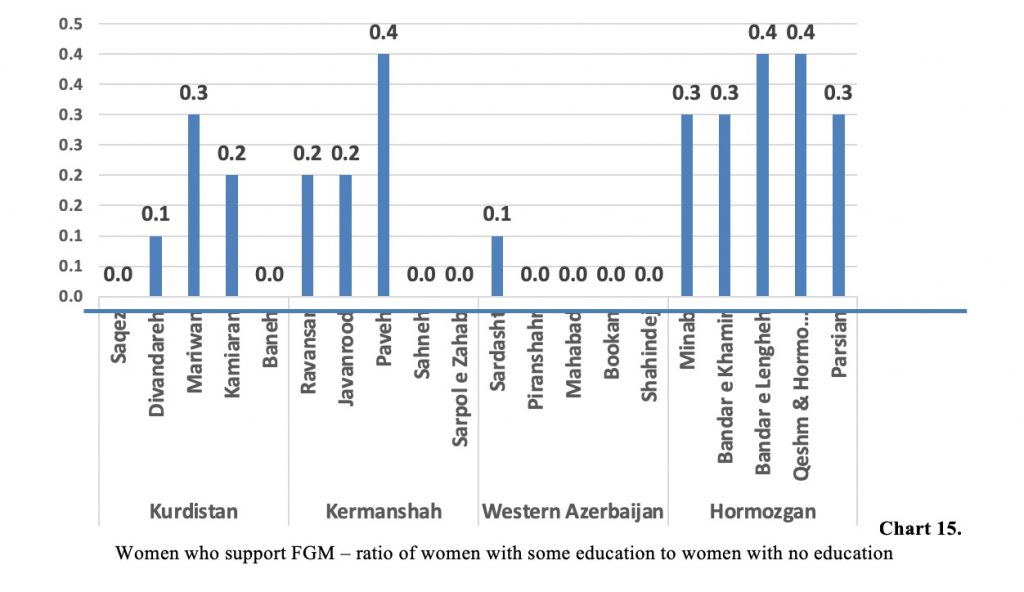
Role of Women’s Education in Support of FGM
Education plays a significant role in shaping people’s opinions and influencing their points of view. In order to gauge whether or not differences in levels of education can affect levels of support for FGM, a survey was carried out in the four selected provinces in Iran.
The findings show that highly educated women are less likely to support the continuity of the practice. The percentages of educated women who support FGM are higher in Hormozgan province, falling between between 11% and 19%. In West Azerbaijan, the level of support for the practice among educated women is very low. Similarly, in Kermanshah province, FGM is supported by 6%, 7% and 18% of women in Javanrood, Ravansar, and Paveh villages, respectively. There is a similar situation in Kurdistan, where some educated women support the continuation of the practice, while the remainder are against it. It shows that education can influence behaviours, attitudes and opinions; however, there are other factors of empowerment which, all together, can make a difference.


Summary of Findings
FGM in Iran is not new; however, the unavailability of data made it practically invisible. Furthermore, the Government was reluctant to admit its existence, and ordinary people were also silent as the whole subject was taboo. Data clearly show that the highest prevalence of FGM can be found in Hormozgan province, although it is also common in a few other provinces in the north-west and west of Iran. The study revealed that FGM occurs in some villages of three western provinces and one southern province. Western provinces are populated by a majority of Sunni Shafi’i, and the southern province of Hormozgan and its islands have significant Sunni Shafi’i communities. Given that the different religious and ethnic groups are dispersed through all these provinces, drawing an exact FGM-affected-area map with rates of FGM is problematic. For example, the practice of FGM in Iranian Kurdistan is patchy and will show sharp variations from one region to another –even from one village to a nearby village.
Most parts of this research had come to a stop by the end of 2014. Despite this apparent setback, much has been achieved over a decade of studying the subject of FGM in Iran. It included travelling over thousands of kilometres, visiting more than 200 villages and interviewing more than 4,000 women and some men from various areas and social classes to collect data about FGM practice. Although this research has not been fully evaluated, our preliminary findings demonstrate that FGM in some selected villages is widespread among women and girls (around 60% in some villages of Qeshm Island) in villages of four provinces in the north-west, west and south of Iran. Within these provinces, however, FGM was not practised in the northern parts of West Azerbaijan, where people are Kurmanji Kurdish speakers, or in the southern parts of Kermanshah and northern parts of Hormozgan.
The real rate of FGM today is something that must be gleaned from the number of new-borns and young children who are being cut. It is a good sign that the prevalence of FGM among women and girls aged 15–29 is lower by 30% than among women aged 30–49, and it appears lower than 8% among children below the age of ten. These points lead us to conclude that the rate of FGM has fallen steadily in the last few decades.
From our interviews with people of both sexes aged 15–49, 38% still support the practice of FGM for reasons of religion, tradition and culture. Such a rate clearly shows that launching immediate intervention and awareness programmes, along with public engagement projects, is urgently required to change attitudes.
Although it is clear that support among younger generations is lower and FGM rates have declined in each of the past ten years, it is difficult to decide whether FGM as a whole is declining quickly. A few important factors in this decline are what we might term ‘modernity’; better access to education; a lack of interest in religion among youth; greater access to all sorts of media, partly through the impact of technology; and the impact of migration from villages to towns (a large number of villagers have secondary homes in nearby towns). What’s more, elderly bibis may not be able to travel around to perform FGM and are not being replaced with a younger generation of practitioners.
To assess whether other regions of Iran are affected by FGM, throughout the fact-finding mission and field work, we continued to identify evidence of FGM in other provinces, such as Ilam, Lorestan, ChaharMahaal and Bakhtiari, Kohgiluyeh and Boyer-Ahmad, Khuzestan, Bushehr, Sistan and Baluchestan, Golestan, Khorasan-e Shomali, Janobi and Razavi, Gilan, and in the more central parts of Iran such as Fars and Yezd. Despite the fact that some Sunni Muslims live in several of the abovementioned provinces, the study revealed no evidence in those locations of FGM.
The study also confirms that there is no evidence of FGM in the following: Sistan and Baluchistan (which has a significant population of Sunni Muslims of the Hanafi sect, Hanafi being the fiqh with the largest number of Sunni Muslims); there is also no evidence of FGM among the forcibly migrated Kurds of Khorasan as well as the Turkmens of Hanafi Muslim of Golestan province; or the small populations of Turkish Sunni Shafi’i groups in Ardabil province and West Azerbaijan province. Interestingly, the Sunni-populated areas of Larestan region, located in Fars province and bordering Hormozgan province, are also FGM free. Furthermore, while there are some large Sunni areas of Hormozgan province itself, such as Bastak and its many villages, which do practice FGM, this is at a much lower rate than in the more the southern regions and islands of the same province.
In the provinces of Khuzestan and Bushehr, FGM was not found among either Sunni Arabs or Shi’a Lur, although there was some evidence of FGM among older women in southern areas of Khuzestan province. FGM was also not found in the provinces of Lorstan, Chahar Mahaal and Bakhtiari, or among the Shi’a Kurds of Ilam, and only in very small numbers in the villages near town of Mehran, which neighbours Kermanshah province: a low rate of FGM was found among women above the age of 50. The study also found that no young girls are now being cut, which indicates that the tradition of FGM has died away in most of the Shi’a communities of both Ilam and Kermanshah.
The research methodology for this study employed mixed research techniques (interviews used both open-ended and closed questions and the data was prepared with a mix of qualitative and quantitative methods). This was because the raw figures cannot give an accurate picture of the actual, on-ground situation. Likewise, when trying to evaluate the impact of even a simple development intervention, the researchers found that it took complex procedures to bring about behavioural changes, which cannot be captured by a single evaluation process. Mixed methods, through the combination of apparent and hidden realities given by the outcomes of qualitative methods, and statistical information provided by the quantitative methodology, produce a comprehensive analysis of the problem (Bamberger 2000).
An example is Chart 10, which shows there is a higher percentage of women who support FGM than men, and women are therefore having the more prominent role in FGM. According to women’s responses to the research questionnaire, the virginity of a woman is of vital importance to secure her future and gain her a good marital status. If a woman can’t protect her virginity, she has ruined the honour of her family. This ultimately overburdens her to preserve the family’s reputation by any means and, to meet that objective, women continue the ritual of cutting throughout the family.
FGM: A Declining Trend in Iran
In some cases, elements of FGM tradition are very evident, but in others (even nearby villages), FGM has been in decline for the past two or three generations. Changing times and modern life, the deaths and non-replacement of bibis, the lack of willingness to accept FGM by the younger generation, education, and the impact of the media, as well as some level of support from clerics, are all factors in the decline of FGM. During the decade of this study, it was observed that the rate of FGM declined every year, for the reasons above and because of the training and awareness-raising campaigns conducted by this study. The following graph demonstrates the reduction of FGM practice during the last six years in Hormozgan, West Azerbaijan, Kermanshah and Kurdistan.

As previously discussed, the prevalence of FGM is declining across the globe, including in the secret pockets in Iran. They are ‘secret pockets’ because the world has very little knowledge of the presence of FGM in these provinces. Within Iran, a very limited number of people, all of whom belong to FGM-affected provinces, have knowledge of its practice in the country.
Chart 16 shows a slow pace of change during the six-year timeframe. The data begin with West Azerbaijan in 2009. During the year 2010–2011, Kurdistan and Kermanshah also showed responses to the wave of change. Hormozgan province, where the prevalence of FGM is the highest in the country, still had a prevalence of more than 60% at the end of 2014, while for the same year, it was 21% in West Azerbaijan, 18% in Kermanshah, and 16% in Kurdistan. It is quite evident from the graph that the process of transformation has been initiated and the affected regions are responding to and adopting change.
Vulnerability Under Human-Rights Laws in Iran
Since the practice of FGM is centuries old and so embedded in the culture and norms of the communities that practise it, it can be difficult for new laws criminalising FGM and the incorporation of measures against FGM into penal codes and existing laws to bear fruit. Because FGM is a taboo in the Middle East, with the exception of Iraqi Kurdistan, there was no official acceptance of the practice’s existence, so enforcing a law against something that does not officially exist is unrealistic.
Nevertheless, there have been some government actions against FGM. For example, Iraq has enacted a law to tackle FGM, especially in the south of Iraqi Kurdistan. The results were minimal at the beginning, but are now improving. Similarly, Egypt still has a high rate of FGM and takes little action against practitioners. The Arab Spring has, however, provided some opportunities to give FGM a higher profile.
In the case of Iran, taking action against FGM is even harder, because there is a lack of support from the Government and a lack of organised NGO groups. Indeed, Iran refused to ratify the Convention on the Elimination of All Forms of Discrimination against Women (CEDAW). During the tenure of President Muhammad Khatami, the Iranian Parliament passed a bill in favour of joining CEDAW, but it was vetoed by Iran’s powerful Guardian Council on the basis that it contradicts Islamic principles.
Nevertheless, Iran has laws that can be used to prosecute and punish mutilation of the body. These include the Women’s Responsibilities and Entitlement Charters on the rights to life, physical integrity, protection against victimisation, mental and physical health and protection against family violence; however, since most of the abovementioned laws are patchily enforced, it is hard to find successful claims made by victims of FGM. In addition, the law does not mention FGM specifically and, therefore, the Islamic law of Iran does not protect women from FGM (Alawi and Schwartz 2015). These laws mean that FGM is carried out in people’s houses by midwives and not by medical practitioners (Alawi and Schwartz 2015).
The lack of information has been coupled with the Government’s denial of the existence of FGM, making it difficult for the issue of FGM to catch the attention of the relevant ministries.
Iran has incorporated some general anti-mutilation laws in its penal code and, according to Article 479 and Article 663 of the Islamic Penal Code, qisas can be invoked when there is cutting of the female genital organs (ARC 2013, Kelly and Breslin 2010). Mutilated persons can also look to the Iranian Protection Law for People with Disabilities, which was enacted in 2003, and the Convention on the Rights of Persons with Disabilities, which became law in 2007. In addition, Iran has ratified the Convention on the Rights of the Child (CRC). Article 2, paragraph 2 of the CRC states that ‘States Parties shall take all appropriate measures to ensure that the child is protected against all forms of discrimination or punishment on the basis of the status, activities, expressed opinions, or beliefs of the child’s parents, legal guardians, or family members.’
Similarly, Article 24 of the CRC puts emphasis on the health of the child, which would be violated if a child is a victim of FGM.
Major Contributing Factors
FGM originated as one form of control over the fidelity of women, particularly when men were away for long time. Salam and De Waal link this to the social acceptance of women by their communities and societies. Often it is governments that violate the human rights of citizens by not properly implementing laws. Similarly, the implementation of many human rights is not possible without the support of the government concerned. However, patriarchal culture and norms often prevail even where the government is trying to do something, especially in the context of women’s and children’s rights, as ongoing FGM in Iran and Egypt shows.
Despite governments’ efforts to ban it and despite many fatwas about the forbidden status of the practice in Islam, FGM is still flourishing (Abiad 2008). In addition to patriarchy, the political structure and system are equally responsible for this. FGM is performed without any direct involvement of men. However, it appears that a large majority of men in the Kurdish and southern areas of Iran are at least aware of the practice.
This ‘disconnection’ of men seems to apply to other ‘women’s issues’, as well. Many studies confirm that men have no knowledge of the reproductive health of women; in most of the societies we are focusing on, it is considered to be a ‘women’s issue’ or ‘secret’ and men have no say in it (Momoh 2005). However, men may be influenced by clerics and imams who preach about the practice as having diverse benefits and a connection with religion. It is interesting to discuss the attitudes of some of the women who have undergone FGM. According to them, those who are not cut are not ‘full women’. For them, FGM is something that needs to be done to bring dignity to both women and girls and to preserve their chastity (Kelly and Breslin 2010). These women do not question FGM as they consider it an old tradition. Importantly, FGM is mostly done when a girl is too young to have any say in the matter. The practice is perpetuated when women put their daughters through FGM as they consider this mandatory for getting married.
More on the Male Perspective
Although FGM is something that happens within the female realm, the role of men cannot be overlooked. Some men take cover behind religion and see any endeavour to end FGM as a Western idea on women’s liberation. In addition, FGM may give men more pleasure because of the tighter vaginal opening and, in most conservative, FGM-practising societies, men refuse to marry uncut girls.
Some Iranian men from practising communities believe that FGM controls women’s sexual drives, and they may say that their community is much purer, with fewer moral problems, compared to Shia Persian or Turkish communities. A common argument used by men in the Sunni populations studied is that, if their women were not cut, they would not be able to control them, which could result in behaviours similar to their Shia counterparts or women in sexually orientated TV programmes or films.
During our study, some men shared that they had sexual intercourse with uncut women from other parts of Iran. They stated that cut women’s genitals are much smoother, smaller in shape, and enjoyable for sex; however, they also claimed that uncut women were better for foreplay. A few of the male interviewees had no knowledge of FGM or whether their wives had been cut. Interestingly, once they were informed of the dangers of FGM and its negative impacts on women’s sexual enjoyment (such that they cannot enjoy sex with their husbands because their clitoris has been partly or fully cut; therefore, they can’t be aroused fully), most confirmed this was the case in their sexual relationships with their wives and said their women were ‘not hot’ or ‘do not give us pleasure’. They also admitted that, to satisfy their sexual desires, they had other sexual partners or simply married a younger second wife. Later they were asked whether, in light of their new knowledge of FGM, they would be willing to have their own daughters cut, therefore suffering the same agony and perhaps being cheated on by their husbands. The interviewees could not answer and instead remained silent and looked away.
References:
Abdollahi, M. and Hosseinbor, M. O. (2002). Baloch students’ tendency toward national identity in Iran. Iranian Journal of Sociology, 4(4), 101–126.
Ahmadi, H. (2018). Ethnicity and Ethnocentrism in Iran: From a Myth to Reality. Ney.
Ahmady, K. (2021). From Border to Border (A comprehensive reach on identity and ethnicity in Iran). Mehri Publishing.
Alamdari, K. (2004). Why has Iran Fallen Behind and the West Progressed? (10th ed.). Towse’a.
Amirahmadi, H. (1998). Ethnicity and Security (H. Shafi’I, Trans.). Strategic Studies Quarterly, 1(2), 207–234.
Ashcroft, B., Griffths, G. and Tiffin, H. (1998). Key Concepts in Post-Colonial Studies. Routledge.
Ashraf, A. (1999). Iranian Identity among Iranians Abroad. (Volume II of Tradition and Modernity). Cultural Bulletin of the Deputy of Financial Affairs of the Ministry of Culture and Islamic Guidance, Tehran.
Atabaki, T. (2002). Azerbaijan and Iranian nationalism. Goftogu: Quarterly on Culture and Society, 33, 17–36.
Baratalipour, M. (2015). Perpetual peace and global political justice. World Politics: A Quarterly Journal, 4(1), 39–63.
Barrington, L. W. (2006). After Independence Making and Protecting the Nations in Postcolonial and Postcommunist States. The University of Michigan Press.
Barth, F. (1969). Introduction. Ethnic Groups and Boundaries. Universitetsforlage.
Bigdeli, A. (2006). Militarist thoughts in the Pahlavi I Era (Part One). www.farsnews.ir/news/8512070023/
Bigdelo, R. (2001). Archaism in Contemporary History. Markaz.
Borujerdi, M. (2000). Iranian culture and identity beyond the borders. Journal of National Studies, 2(5), 317–330.
Brown, G. K. and Arnim, L. (2010). Conceptualizing and Measuring Ethnicity. Oxford Development Studies, 38(4).
Brown, R. (1996). Social Identity. In A. Kuper and J. Kuper (Eds.), The Social Science Encyclopedia. Routledge.
Buurih, J. (1997). Culture Identity and Immigration. Ethnic and Racial Studies, 21, 574–601.
Cashmore, E. (1996). Dictionary of Race and Ethnic Relations (4th ed.). Routledge.
Castells, M. (2010). The Information Age: Economy, Society and Culture (A. Aligholiyan and A. Khakbaz, Trans.). Tarhe No.
Coughlan, R. (1985). Ethnicity and the State: Five Perspectives. Choice.
Diakonoff, M. M. (2004). History of Ancient Iran (R. Arbab, Trans.). Scientific and Cultural.
Sanie Ejlal, M. (2005). An Introduction to Iranian Culture and Identity. Institute for National Studies.
Entman, R. and Rojecki, A. (2000). The Black Image in the White Mind: Media and Race in America. Chicago University Press.
Eriksen, T. H. (1993). Ethnicity and Nationalism. Pluto Press.
Faulks, K. (2000). Citizenship. Routedge.
Fenton, S. (2004). Beyond Ethnicity: The Global Comparative Analysis of Ethnic Conflict. International Journal of Comparative Sociology, 45(3–4). https://doi.org/10.1177/0020715204049592
Fuller, G. (1993). The Center of the Universe (A. Mokhber, Trans.). Markaz.
Ghasemi, A., Khorshidi, M. and Heidari, H. (2011). Harmony between national and ethnic identity in Iran and Iranian ethnic groups’ approach toward national unity and the right to their destiny. Quarterly of Social Sciences, 18(55), 57–92.
Giddens, A. (2006). Sociology (M. Saburi, Trans.). Ney.
Giddens, A. (2019). Modernity and Self-Identity (N. Movaffaghiyan, Trans.). Ney.
Graves, S. (1999). Television and Prejudice Reduction: When Does Television as a Vicarious Experience Make a Difference? Journal of Social Issues, 55(4), 707–725.
Haghpanah, J. (2003). Formulation procedure of ethnic policies in the Islamic Republic of Iran. Strategic Studies Quarterly, 6(91), 462–542.
Hall, S. and Gieben, B. (1990). Formation of Modernity. Polity Press.
Hassanpour, A. (1992). Nationalism and Language in Kurdistan. Mellen Research University Press.
Hechter, M. (1975). Internal Colonialism: The Celtic Fringe in British National Development, 1536–1966. Routledge & Kegan Paul.
Jenkins, R. (2014). Rethinking Ethnicity. Sage.
Kachooyan, H. (2008). Evolutions of Identity Discourses in Iran. Ney.
Kasravi, A. (1978). Eighteen-Year History of Azerbaijan. Amirkabir.
Kaufmann, E. (2015). Land, History or Modernization? Explaining Ethnic Fractionalization. Ethnic and Racial Studies, 38(2), 193–210.
Khamei, A. (2002). Pan-Turkism and its scientific and historical value. Socioeconomic Information, 17(81 and 82), 40.
Kurung, S. (2002). Democratization of international relations. Gozareshe Goftogu. 1(2), 36–44.
Malesevic, S. (2004). Sociology of Ethnicity. Sage Publication Ltd.
Malesevic, S. (2011). The Sociology of Ethnicity (P. Dalirpur, Trans.). Ameh.
Milton, M. G. (1964). Assimilation in American Life. Oxford University Press.
Mirmohamadi, M. S. (2011). A comparison of perpetual peace in Kant’s human-oriented thought and just peace in Shia thinkers’ thought. Ma’rifat-e Adyan, 2(4), 117–146.
Motyl, A. (2004). Middle East: Encyclopedia of Nationalism (K. Fani and M. Mohajer, Trans.). Library of the Ministry of Foreign Affairs.
Mozafari, A. (2012). Ethnicity and social security: A case study of the Baloch residing in Sistan and Baluchistan Province. National Congress on Border Cities and Security:Challenges and Strategies. Nesher Seyaset.
Muir, R. (1997). Political Geography – A New Introduction. Mac Millan Press Ltd.
Nagel, J. and Olzak, S. (1982). Ethnic Mobilization in New and Old States: An Extension of Competition Model. Social Problems, 30(2), 127–143.
Oldfield, A. (1990). Citizenship and Community: Civic Rebublicanism and The Modern World. Routledge.
Olson, E. T. (2002). Personal Identity. In E. N. Zalta (Ed.), The Stanford Encyclopedia of Philosophy.
Olzak, S. (1985). Ethnicity and Theories of Ethnic Collective Action. Research in Social Movements. Conflicts and Change, 8, 65–85.
Qayyim, A. (2001). A sociological study of the life and culture of the Arab in Khuzestan. Journal of National Studies, 2(7), 15–226.
Popper, K. (1962). The Open Society and its Enemies.
Ramezanzadeh, A. (1998). Ethnic crisis trend in Iran. Strategic Studies Quarterly, 1, 217–228.
Rashidi, H. (2008). Investigation of the Relationship between Social Factors and Collective Identity (Ethnic, National, and Global) among Students at Islamic Azad University of Mahabad [master’s thesis]. Islamic Azad University of Tabriz.
Ruz, F. (2005). Modern Fascination: Multifold Identity and Mobile Thought (F. Valiyani, Trans.) (4th ed.). Aras Publishing.
Sanaz, A. (1997). Development and ethnic challenges, development and public security. Conference on Public Development and Security. TSB.
Shayegan, D. (2002). Mental Idols and Primordial Memory. Amirkabir.
Schwarzmantel, J. (2003). Citizenship and Identity: Towards a New Republic. Routledge.
Solomos, J. (1986). Varieties of Marxist Conceptions of Race, Class and the State: A Critical Analysis. In J. Rex and D. Mason (Eds.), Theories of Race and Ethnic Relations. The Oxford University Press.
Tavassoli, G. (2019). Sociological Theories. Samt.
Turner, J. H. (1998). The Structure of Sociological Theory (6th ed.). Hadsworth Publication.
Vali, A. (2018). Speech at the Birthplace of Kurd Nationalism. Cheshmeh Publishing.
Yusofi, A. (2001). Interethnic relations and their effects on the identities of the ethnic groups in Iran. Journal of National Studies, 2(8), 11–42.
Weber, M. (1968). Economy and Society. University of California Press.
Zokaei, M. S. (2002). Citizenship ethics: The relationship between collective identity-seeking and altruistic values. Bulletin of the Iranian Sociological Association, 5.